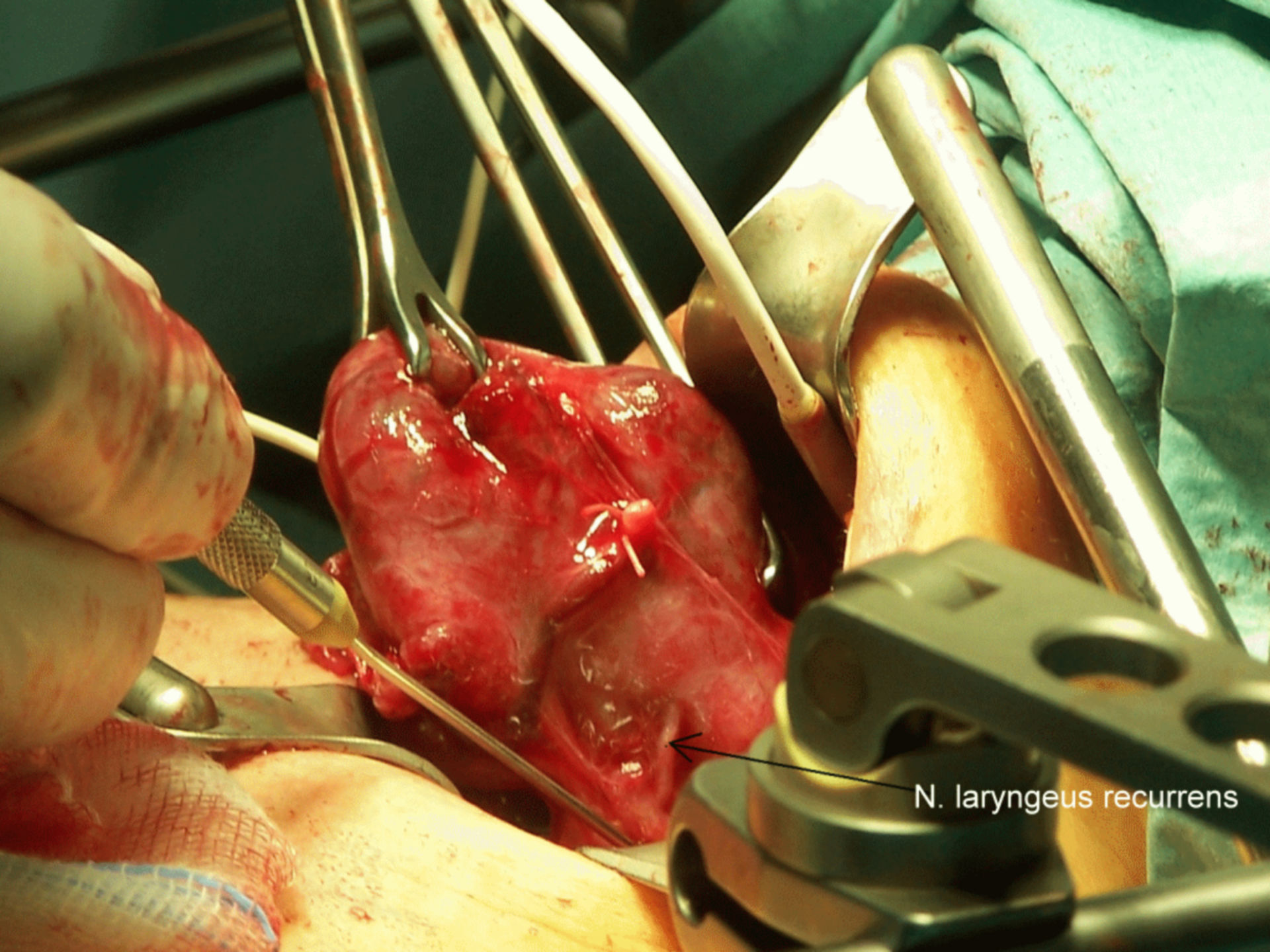
The left N. laryngeus recurrens is completely displayed, its function is tested via neuromonitoring (probe).
A thyroidectomy is conducted under general anesthesia. For operational access to the thyroid, a horizontal skin incision (Kocher transverse collar incision) is made app. 3 cm above the jugulum. It is placed in a skin fold for a better cosmetic result. In sequence, subcutis, platysma and superficia neck fascia are split. The straight neck muscles are split in the median line. After that, the preparation of the thyroid can begin.
In rare cases, a sternotomy may be required, for exampe in extremely large retrosternal (respectivey intrathoracic) goiters, or when a restrosternal lymphadenectomy is necessary.
During surgery, is is important, especially in extensive resections, to carefully prepare and preserve the parathyroids and the Nervus laryngeus recurrens (see complications). The nerve preparation can be observed by neuromonitoring during surgery.
Source: THWZ