The biggest problem with many orphan diseases is their diagnosis and ALS is no exception. Patients may wait over a year for diagnostic certainty – with a median survival rate of 30 months, this is unacceptable. What can be done?
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease, which affects motor neurons in the brain and spinal cord. It is the most frequent motor neuron disease; the course of disease is progressive and ultimately leads to death. Because of the diverse, slowly developing and – in the beginning – often subtle symptoms, diagnosing ALS early is a diagnostic challenge. Recently, a review regarding the problem of delayed diagnosis in ALS was published in the European Journal of Neurology.
In the included studies, mean diagnostic delay from first symptoms noticed by the patient to definitive diagnosis was between 9 and 24 months. For most ALS patients more than a year goes by until they have diagnostic certainty. With a median survival time of approximately 30 months, this time span constitutes a significant part of the whole disease course, although about 10–15 % of ALS patients survive for more than ten years after symptoms begin. While there is no cure for ALS, providing multidisciplinary care, including respiratory management, pharmacological treatment with riluzole, nutritional management, and symptomatic therapies, has been shown to improve quality of life and survival rates. Therefore, an earlier diagnosis can open doors to timely therapeutic interventions, offering hope and tangible benefits to ALS patients and their families.
The authors of the review tried to understand the reasons for delayed diagnosis. They split up the time span from first symptoms to final diagnosis in two parts. The first part of diagnostic delay was defined as the time from the moment the patients are noticing their first symptoms to the first doctor’s visit. Patient-related factors mainly influenced this period. Many patients wait for half a year or more before they visit their doctor with their symptoms caused by ALS. Patient characteristics like personality traits, psychological comorbidity, age and socioeconomic factors influenced the extend of delay. For example, a lower income was associated with a longer delay to the first medical visit.
The second part of diagnostic delay was defined as the time from the first presentation to any physician (usually primary care physician) to the definitive diagnosis of ALS. In this second part of diagnostic delay, physician-related factors played a larger role. Due to the rarity of the disease and the often subtle and variable early symptoms, primary care physicians may not immediately suspect a neurological condition. As a result, they may refer the patient to other specialist doctors, such as ENT specialists, orthopedists, or rheumatologists, as they attempt to identify the underlying cause of the symptoms. However, the review found that patients who were promptly referred to a neurologist after their initial physician’s visit received their ALS diagnosis much earlier compared to those who were initially referred to a doctor of another specialty. This highlights the crucial role of clinical suspicion and early involvement of neurologists in the diagnostic process, as their expertise is vital for accurate and timely diagnosis of ALS.
Depending on the most pronounced symptoms in the beginning of the disease course, there are two main subtypes of ALS. Spinal ALS is the most common ALS subtype; it presents with asymmetric paresis of the extremities and accounts for about two thirds of ALS cases. In Bulbar ALS (about one third of ALS cases), the most pronounced symptoms are dysarthria and dysphagia. Rarely occurring is another ALS subtype, respiratory ALS, which affects respiratory muscles from the start, leading to symptoms like exercise-related shortness of breath. The ALS subtype has a substantial impact on the extent of diagnostic delay. In the case of Bulbar ALS, the time to diagnosis was notably shorter, ranging between 7 to 10 months. The authors of the review attribute this relatively shorter delay to the typically faster progression of Bulbar ALS. The pronounced symptoms affecting speech and swallowing often prompt patients to seek medical advice earlier in the disease course, expediting the diagnostic process.
On the other hand, Spinal ALS tends to be associated with a longer diagnostic delay, ranging from 10–22 months. The slower progression of motor symptoms in the limbs might lead some patients to initially dismiss or downplay the early signs, delaying medical consultation. In Spinal ALS, the first physician that patients visit particularly often refers them to specialists other than neurologists, which adds to diagnostic delay. The presenting paresis of the extremities often leads to a first differential diagnosis of a spine-related issue, causing patients to be referred to orthopedists or neurosurgeons. As a result, more than half of patients are diagnosed with a condition different from ALS on their diagnostic journey. The most common diagnoses, that were later found to be false, were degenerative spine disease and peripheral neuropathies. 3–10 % of patients with spinal ALS even underwent surgical procedures meant to help with symptoms that were later attributed to spinal ALS.
Even when the patient is referred to a neurologist immediately, diagnosis remains challenging. The list of neurologic differential diagnoses is extensive, most important conditions with similar symptoms are spondylotic myelopathy, myasthenia gravis, chronic inflammatory demyelinating polyneuropathy (CIDP), multiple sclerosis and cerebrovascular disease.
The diagnosis of ALS relies on a comprehensive and integrated approach, combining multiple diagnostic tools to establish a conclusive assessment. Medical history and physical examination serve as crucial initial steps in this process, while imaging studies play a significant role in excluding potential differential diagnoses. Additionally, complex and time-consuming electrodiagnostic studies, such as nerve conduction studies and electromyography, are indispensable for achieving an accurate ALS diagnosis. According to diagnostic criteria for definitive ALS, examination needs to show dysfunction of the upper motor neuron and lower motor neuron in at least two distinct regions of the body.
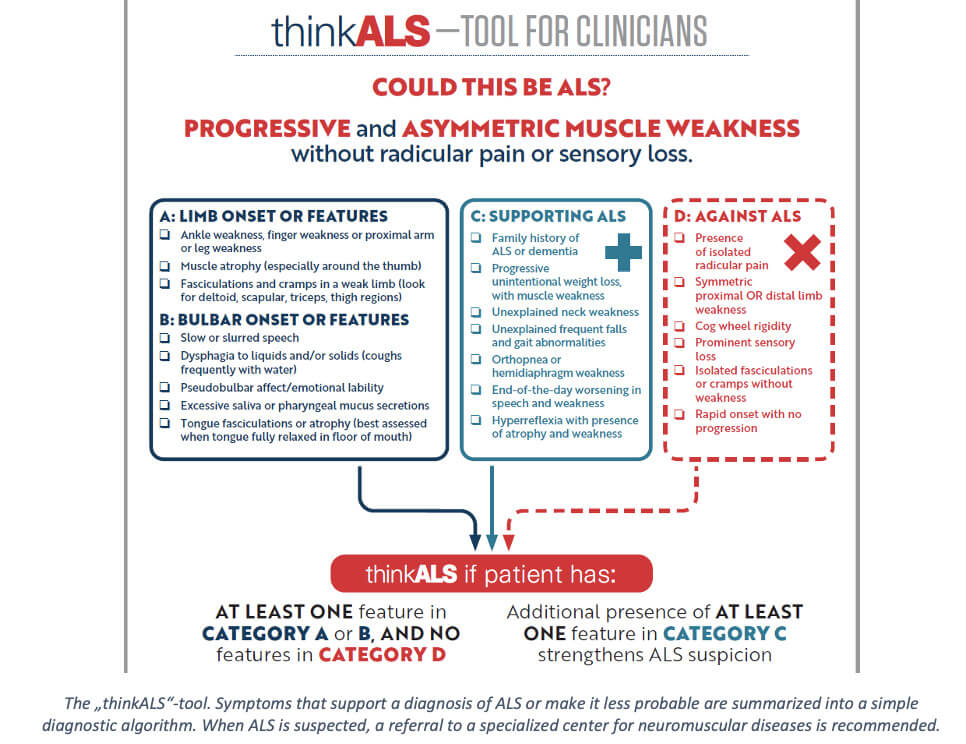
In the study, diagnostic delay in ALS did not differ significantly between different national health care systems and there was no evidence of improvement in recent years, underscoring the urgent need for action to expedite the diagnostic process. To address the problem, the American ALS Association developed the thinkALS-tool. It serves as a diagnostic guide and helps in quickly determining if ALS could be the underlying condition responsible for the presenting symptoms, which in turn should lead to referral to a specialized center.
While tools like this show great promise in streamlining ALS diagnosis, their efficacy hinges on one crucial factor: the physician’s awareness of ALS as a potential explanation for the presenting symptoms. Although the ALS Ice Bucket Challenge of 2014 succeeded in capturing global attention and supporting ALS research, the disease’s rarity still presents a challenge in keeping ALS on the clinical radar.
Image Source: Major Tom Agency, Unsplash