Many patients are flabbergasted when they see an image of the tumor I removed from their body. It’s remarkable when you think about all of the tissues, cells, and organs packed inside each of us. My favorite surgical space, the abdominal cavity, contains a remarkable array of organs including the stomach, small/large intestine, kidneys, pancreas, spleen, bladder, and my favorite organ, the liver.
The liver includes the gallbladder and bile ducts. Occasionally, patients are diagnosed with a massive tumor at some site in their body. Sarcomas arising in the retro-peritoneum, the area behind the gut where the kidneys, aorta, vena cava, and some significant muscles and nerves reside can be larger than a basketball. Patients and family members are astonished a tumor can grow to a relatively huge size before being detected after causing mild discomfort or other subtle symptoms.
Gastrointestinal stromal tumor (GIST) of 20 cm in diameter
A few weeks ago, a new patient came to my office with a giant tumor. She is a patient in her early 70’s who has been healthy and active. She takes a single medication for her mild hypertension, which controls and normalizes her blood pressure. She and her several daughters noticed she was becoming less active and more easily fatigued over the past four or five months. Blood tests obtained during a visit to her family physician one month ago revealed a red blood cell count only about half of normal; she was severely anemic. The patient noted she was not eating well and her abdomen felt “swollen”, so the physician referred her to a gastroenterologist for endoscopy and ordered a CT scan. The CT scan was obtained before the endoscopy, and a very large tumor of the upper abdomen, greater than 20 cm in diameter, was readily evident. The gastroenterologist performed a colonoscopy, which showed no abnormalities or sources of bleeding, while an upper endoscopy revealed a small area of ulceration along the final third of the stomach. Biopsies were obtained of this area, which ultimately demonstrated a gastrointestinal stromal tumor (GIST). The patient was then referred to me.
This soft spoken, delightful lady and her daughters agreed to allow several medical students and residents examine and palpate her abdomen. When she lay supine on the examining room table, it appeared she had an approximately full term pregnancy with a mass palpable from the tip of her sternum extending well below the umbilicus (belly button).
The residents, medical students, and I reviewed her CT images. In addition to the large mass arising from the greater curvature of her stomach, there were two 4 cm metastases in her left liver and one similar size lesion in the right liver. GIST frequently metastasizes to the liver. These tumors can be treated with a medication called imatinib, a drug targeted to a specific genetic gain-of-function mutation in a tyrosine kinase receptor called c-KIT. This patient had already been started on oral imatinib, but she was extremely symptomatic with poor appetite, early satiety, and was requiring weekly blood transfusions for persistent bleeding from the ulcerated stomach tumor. I had a long discussion with the patient and her daughters, and after answering all questions and discussing alternatives, they agreed to an operation early the next week to remove the malignant stomach tumor and treat the three large liver metastases.
Removal of the giant tumor
A few days before the operation we transfused the patient with two units of packed red blood cells because her hemoglobin level, which should be 12-15 gm/dL, was only 6.5 gm/dL the day I saw her in clinic. We started the operation with an incision from the tip of her sternum, called the xiphoid, to her belly button. Upon entering the peritoneal cavity, the soccer-ball size mass protruded from the incision. As expected from the endoscopy and CT findings, despite the large size of the tumor, it arose from a short segment along the lower aspect of the stomach. Working with a chief resident, we dissected this sizable tumor free from the surrounding structures adherent to it, including the pancreas, duodenum, and the transverse colon. Once the tumor was dissected free from all of these structures, it was a simple matter of firing a gastrointestinal stapling device twice along the greater curvature of her stomach assuring we were clear of the malignant tumor. The tumor and a small volume of her stomach was removed entirely.
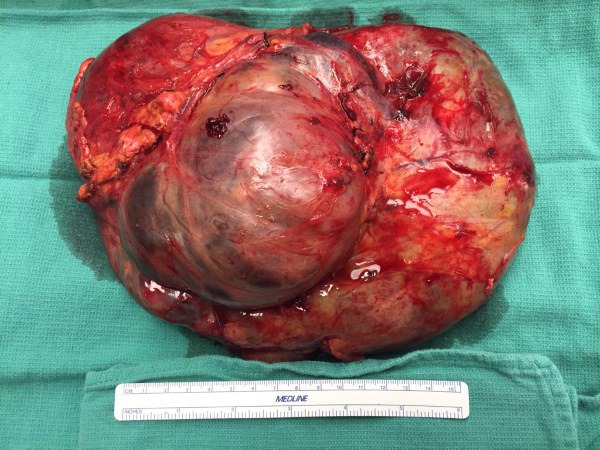
Removed gastrointestinal stromal tumor (GIST) of 23 cm in diameter.
Earlier in my career, if I wanted a picture of a tumor or a photograph during an operation, I had to arrange for a certified medical photographer to join us in the operating room. One of the joys and advantages (or disadvantages) of modern technology is all surgeons are now their own photographer using their cellular telephones. Patients, including this lady and her daughters, often ask me to take a picture to show them the offending malignancy. I wanted to take the large stomach tumor over to pathology myself, so I removed my surgical gown and gloves and took a couple of quick cell phone photos of the tumor with a sterile measuring tape placed below it to provide a size reference. I never place any patient names or numbers in these photos, and I always delete the images from my phone after sharing them with the patient and their families. Patient privacy and confidentiality must be conserved and respected!
I carried the bucket containing the gastric GIST over to pathology, and our pathologist confirmed the resection margins were tumor-free. I scrubbed my hands again and re-gowned and gloved. We removed the left liver containing the two large tumors. Intraoperative liver ultrasound revealed about a dozen small tumors (3-4 mm) scattered throughout liver. This was not an unexpected finding with a GIST, and I knew treatment with imatinib could successfully control these small tumors for many years. The larger tumor in the right lobe was deep in the liver, but was easily destroyed completely using ultrasound-guided microwave ablation. At the conclusion of the operation, it was easy to sew close the abdominal wall muscles because there was no longer a large tumor protruding and pressing outward.
“Do you have pictures of Mom’s cancer?”
I walked out to speak with the patient’s daughters and described the findings and results of the operation. I reported their mother was stable and did very well throughout the operation. She required no blood transfusions and was resting comfortably in the recovery room. The eldest daughter finally asked the question I expected, “Do you have pictures of Mom’s cancer?”
I hesitated briefly as a few of the daughters squirmed or grimaced, and then responded, “In fact, I have some on my phone. Be careful what you wish for; are you sure you want to see this?”
After quickly exchanging glances among themselves, all agreed they wanted to see photos revealing the appearance of the large tumor corresponding to the CT images I had shown them in the office. I opened the photos on my phone and was met with common exclamations of disbelief and incredulity. The usual questions ensued, “Oh my God, how can some thing like that grow in our mother?”
“How could she be walking around with that thing in her?”
“You said that thing is 23 cm in diameter. What is a centimeter? How many inches is that? How on earth can something that big not just kill you outright?”
All good questions ladies. I converted centimeters into inches for them, but still sensing some uncertainty, I finished the conversion for them by saying, “Surgeons like to compare the size of tumors to common objects like food. Your mother had the equivalent of a large canteloupe melon in her belly.”
The whole family was stunned. As more family members arrived, each wanted to see the pictures of the incomprehensibly large GIST. Low whistles, exclamations of amazement, or grunts of distress and disgust emitted from each individual who saw the images.
Happy ending
Happily, this delightful lady recovered from her operation quickly and uneventfully. On the evening of surgery she grasped my hand, and eyes brimming with tears, thanked me for removing the large mass. She stated unequivocally she felt better than she had in months, and the sensations of heaviness, pressure, and discomfort had vanished. She had minimal pain from her abdominal incision and was discharged from the hospital four days after the procedure. When I saw the patient and several of her daughters back in the office for her first post-operative visit, they asked for more details about the tumor. I reported, like a pediatrician would do with a newborn baby, the pathologist had weighed her tumor. It came in at a whopping 2.3 kilograms, or just over 5 pounds! Despite the presence of stage IV disease with several remaining small liver metastases, this patient in all probability will live many more years thanks to the availability of the targeted drug imatinib. The patient now has a slightly concave rather than a very protuberant abdomen, and she is able to eat full-sized meals and enjoy her children and grandchildren.
Keep reading:
That Thing Was Growing Inside Me? (Part 1)
That Thing Was Growing Inside Me? (Part 3)