The tumor I was talking about in my last piece was big, but is not my personal record for largest tumor removed. I am certain I have colleagues who could easily describe tumors larger than the biggest one I ever resected. Sarcomas in particular can grow to a relatively enormous size in many locations in the body.
Slightly more than a decade ago, I received a phone call from a panicked primary care physician from a small town in West Texas. The physician rapidly and breathlessly explained a patient came into his office two days before stating he was unable to eat, his waist size had increased from 34 to a 52 inches in only a few months, and the perfunctory CT scan revealed a mass extending all the way from the liver down into the pelvis.
An abdomen about to burst
I immediately accepted the patient and told the physician to send him to my office the next day. This 50 something year old gentleman, who had been previously completely healthy and an active, hard working farmer, was clearly miserable. His abdomen was distended to the point of looking like it was going to burst. The abdominal skin was taut and shiny, and he was breathing over 30 times a minute because he was unable to take a deep breath from the increased pressure upward on his diaphragm and lungs. The muscles of his arms, legs, and face were wasted. He had a typical appearance of cachexia; severe malnutrition with his pleading eyes protruding from sunken sockets.
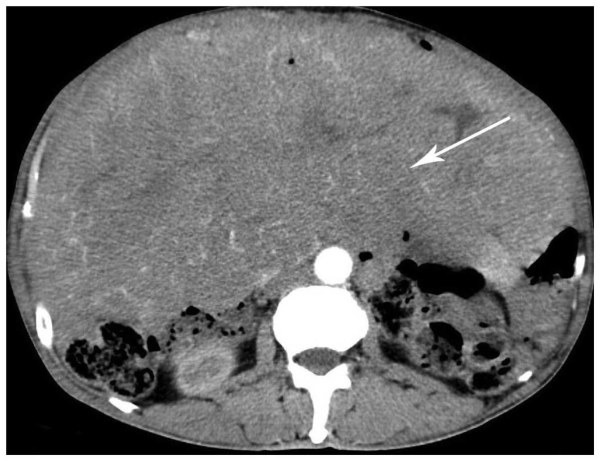
After speaking with this gentlemen and his family and completing a physical examination, I reviewed the CT images obtained in West Texas. I realized his massive tumor was originating from the edge of the right lower liver, extending down into his pelvis and compressing the stomach, all of the small and large intestine, and even causing compression of the bladder and ureters, the small tubular structures draining urine from the kidneys to the bladder. Despite the relatively immense size of this tumor, it was clear it arose from the lower edge of the liver and was not near any of the major blood vessels flowing into the liver or draining blood out of the liver.
Image of a giant peritoneal sarcoma compressing the intestines.
“Bye bye, tumor!”
I scheduled this man for an operation only two days later because of his debilitating symptoms. I started the operation with a right subcostal incision, a cut in the skin under the ribs on the right side. A quick assessment confirmed the tumor was arising from a small portion of the liver lateral to the gallbladder. Intraoperative ultrasound confirmed there were no major blood vessels involved by the tumor. It was possible to remove a small section of the liver from which the tumor arose, less than 10% of the total liver volume, and then detach the tumor from other abdominal organs. The tumor was so large I had to extend the incision simply to remove it from the abdominal cavity. To my surprise, the tumor had very few attachments to other organs or structures, and once its origin in the liver was divided, I was able to gently deliver the mass out of the peritoneal cavity and clamp and divide the few remaining blood vessels supplying the tumor.
“Holy shit, what is that thing?”
This tumor was so large and somewhat gelatinous I was concerned I would drop it or rupture it. We did not have a basin or container large enough to transport the tumor from the operating room to the pathology suite. Therefore, the circulating nurse brought a wheeled cart into the operating room usually used to transport sterile instruments and supplies from the surgical core area to the operating room. We wrapped the tumor in sterile towels and I pushed it over to the pathology suite. The wide-eyed expressions from the experienced senior pathologist and the surgical pathology staff were hilarious. The pathologist took one glance as I uncovered the tumor and exclaimed, “Holy shit, what is that thing?” Why does everyone keep calling these giant tumors “things”?
I showed the pathologist the origin of the tumor from the edge of the liver and returned to the operating room. The intestine and other structures, which had looked compacted, blue, and pathetic, were already pink and contracting wildly. It reminded me of times when I found myself in a large, relatively immobile crowd of people, and the wonderful feeling of relief once I broke free from the crowd and could move unencumbered. We had plenty of room to spare closing his abdominal wall muscles and the skin.
This gentleman was one of the happiest people I’ve ever seen on the morning of his first post-operative day, despite a long bilateral subcostal incision. He was already wolfing down breakfast of eggs, pancakes, and sausage he had gone to the cafeteria to purchase. We had not yet written an order allowing him to drink even liquids. Absence of a formal medical order permitting him to drink broth and juice or enjoy jell-o in any color he ordered was not going to stop him; he had room for his stomach to distend and his bowel to work and he was not going to wait around for us. He explained he was making up for lost time and was going to eat whatever he wanted. Fortunately, he suffered no ill effects from his rapid self-progression to a regular diet. He was discharged from the hospital four days after the operation. When I saw him back for his first post-operative visit five days later, we discussed the rare hepatic angiosarcoma I had removed. I informed this man and his family I had delivered a 45 cm greatest diameter tumor, almost 18 inches in size. The final weight of the cancer emanating from his liver was 6.5 kilograms, or slightly greater than 14 pounds. The pathologist admitted the total tumor weight was probably greater because when he cut into it a large amount of fluid and old blood drained from the tumor. I estimate after lifting it from the patient’s abdominal cavity to the back table in the operating room it seemed like at least 20 pounds to me.
Sarcomas: Numerous operations, recurrent tumors
Sarcomas are unusual and uncommon cancers with a propensity to recur locally or metastasize to the liver and lungs. Individuals who are experts in sarcoma surgery will say sarcoma patients can train new surgeons for many years because of the numerous operations they may require for multiple recurrences. In general, chemotherapy is not particularly effective for types of sarcoma other than GISTs. This gentleman did well for almost four years before he developed recurrent tumors in his peritoneal cavity. I operated and removed these intra-abdominal tumors, and he did well for another two years before he developed a few lung metastases. These pulmonary tumors were removed during two operations over the next year; but the patient ultimately succumbed to multiple new tumors growing in his lungs. Near the end of his life, he declined chemotherapy treatments when he learned the low probability of success in shrinking the tumors and the profoundly toxic side effects. He did achieve over six years of what he proclaimed, “A really great life.” He was upbeat, energetic, ate normally, ran his farm, loved to tell jokes, and travelled extensively with his wife and family. He told me the experience with cancer taught him to enjoy every day he was granted. After the initial huge tumor was removed, he was quickly able to eat and exercise and return to his normal appearance and level of activity.
When our senses don’t sense it
Biology is remarkable. The complexity of the human body is difficult to comprehend. There is much we still do not know or fully understand. The development of cancer is an equally complicated process with a mind-boggling interplay of genetics, epigenetics, biochemistry, immunology, and dynamic interactions with the host. The occasional patient we see with massive tumors represents an eye-opening experience for all involved; it is difficult to believe how large a tumor can grow to be in some locations in a human body before causing symptoms leading to detection.
When the inevitable question is asked by patients and family members after I remove a very large tumor, the answer is, “Yes, incredibly enough, that ‘thing’ was really growing inside you.”
And as amazing and wonderful as our primary senses are, I cannot explain why a tumor can grow to a massive size before we sense something is awry.
Keep reading: That Thing Was Growing Inside Me (Part 1)That Thing Was Growing Inside Me (Part 2)